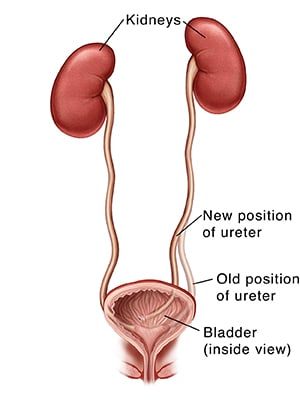
The ureters are the tubes that carry urine from the kidneys to the bladder. The connection where one or both of your child's ureters attach to the bladder isn't fully developed. This can cause urine to flow from the bladder back up into the kidney. This is called vesicoureteral reflux (VUR). VUR doesn't cause pain. But it can increase your child's risk for urinary tract infections (UTIs). Over time, it can also damage your child's kidneys.
With ureteral reimplantation surgery, one or both ureters are moved. This makes their connection to the bladder stronger. It also helps the urine drain well and not flow backwards.
Getting ready for surgery
Prepare your child for the surgery as told. Also be sure to:
- Tell the doctor about any medicines your child takes. Your child may need to stop taking some or all of them before surgery, as directed by the doctor.
- Follow any directions your child is given for not eating or drinking before surgery.
The day of surgery
The surgery takes about
Before the surgery begins:
- An I.V. (intravenous) line is placed in a vein in your child's arm or hand. This line supplies fluids and medicines (such as antibiotics).
- To keep your child from feeling pain during the surgery, general anesthesia is given. This medicine lets your child sleep through the surgery. A tube may be put into your child's throat to help with breathing.
- A thin tube (catheter) may be placed into your child's bladder to drain urine.
During the surgery:
- The surgery is done as an open surgery, as a robotic-assisted laparoscopy, or through an endoscope. The end of the ureter and some muscle near it are detached from the bladder.
- The surgeon will decide where in the bladder to reimplant the ureter. A tunnel is then made for the ureter to be placed inside.
- The ureter is moved to the new site in the bladder and put into the tunnel.
- Once the ureter is in place, it is secured with stitches.
- If the other ureter is also being treated, it's done at this time.
- The bladder is stitched closed.
- Any skin incisions made in the belly are closed with stitches or surgical tape.
- A small tube (drain) is placed near the incision. This drain removes fluid that can build up after the surgery.
Recovering in the hospital
After the surgery, your child will be taken to a recovery room. There your child will be watched as the anesthesia wears off. At first, they may feel sleepy, nauseated, and have a sore throat (if a breathing tube was used). If needed, medicine will be given to manage pain. When your child is ready, they will be moved to a hospital room.
The urinary catheter will be removed before your child leaves the hospital. The drain may also be removed. If the child is sent home with the drain, you will be shown how to care for it at home.
Recovering at home
Follow the doctor's instructions for how to care for your child at home. Be sure to:
- Give your child medicine as directed.
- Care for your child's incision and drain as instructed.
- Follow the doctor's guidelines for bathing your child.
- Don't let your child be active until the doctor says it's okay.
- Ask the doctor when your child can return to day care or school.
When to contact your child's doctor
Call your child's doctor right away if your child has:
- A fever of
100.4°F (38°C) or higher, or as advised by the doctor. - Symptoms of infection at an incision site (such as increased redness or swelling, warmth, worsening pain, or bad-smelling drainage).
- Problems with the drain.
- Severe vomiting.
- Dark blood or clots in the urine (some pink-tinged urine is normal).
- Problems with being able to urinate.
- Crying that can't be calmed or refuses to feed (infants).
Call 911
Call
- Chest pain.
- Trouble breathing.
Follow-up
At follow-up visits, the doctor will check how well your child is healing. If needed, your child's stitches and drain will be removed in about
Risks and possible complications
All procedures have some risk. Possible risks for this surgery include:
- Bleeding (your child may need a blood transfusion).
- Infection.
- Pain.
- Urine leakage from the ureters.
- The stricture of ureters comes back.
- Damage to the bladder, bowels, or other organs.
- Kidney damage.
- Risks of anesthesia (the anesthesiologist or nurse anesthetist will discuss these with you).
Featured in
Online Medical Reviewer: Donna Freeborn PhD CNM FNP
Online Medical Reviewer: Marc Greenstein MD
Online Medical Reviewer: Raymond Kent Turley BSN MSN RN
Date Last Reviewed: 09/01/2025
© 2000-2026 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.Related Articles

Ureterolysis
Pressure from a mass of tissue or scar tissue is blocking one or both of your ureters. This causes urine to back up into the kidneys instead of flowing out of the body. Ureterolysis can help treat this problem. With this surgery, the ureter is freed from the tissue that is pressing on it. The ureter is then moved to a new position away from the blockage. Read on to learn about this procedure.
Pyeloplasty
Pyeloplasty is surgery to unblock the ureter and allow urine to flow again. Read on to learn more about the surgery and what to expect.
Ureteral Stricture Surgery (Ureteroplasty)
Ureteroplasty is surgery to remove a narrowing (stricture) in the ureter. Learn what to expect with this procedure.
Distal Ureterectomy
Cancer has been found in the lower (distal) part of one of your ureters. To treat the cancer, distal ureterectomy is done. This surgery removes the lower part of the ureter and part of the bladder. Read on to learn more about this procedure and what to expect.

